Volleyball protection knowledge: biceps femoritis
  
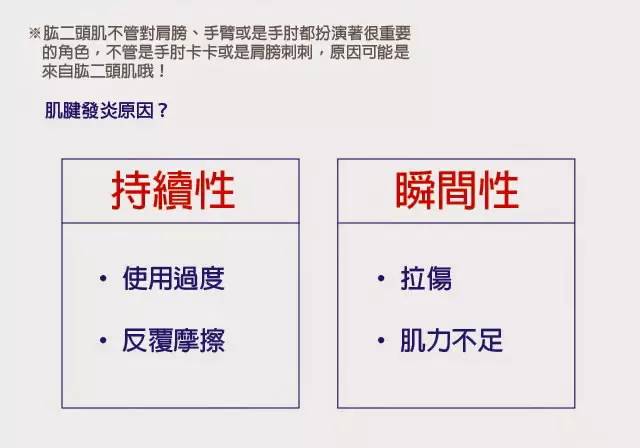
What is biceps tendonitis?The biceps brachii muscles are lifted from the superior scapular humerus and pass through the fibrous fiber conduit formed by the intercondylar sulcus and transverse ligament. When the shoulder joint is extended, adducted, and rotated, the tendon slides upward; when the shoulder joint flexes, abducts, and rotates outward, it slides downward. When the upper limb flexes the elbow in the outreach position, the biceps tendon tends to wear, and long-term friction or excessive activity can cause congestion, edema, and thickening of the tendon sheath, causing acute edema or chronic injury inflammation of the tendon sheath synovial layer, resulting in paralysis. The biceps muscle tendon has a sliding function in the tendon sheath, which causes clinical symptoms, called biceps tendonitis or tenosynovitis. Volleyball, badminton and other athletes often suffer from this disease, which is one of the common causes of shoulder pain due to acute onset of trauma or strain. Its clinical manifestations are mainly shoulder pain, tenderness, and limited shoulder joint activity. If not treated in time, it can develop into frozen shoulder.
Biceps, function and starting and ending points

Q: Why do you need to know the starting and ending points of muscles?
A: The starting and ending points of the muscles are all parts that are prone to injury and cause inflammation. Knowing the starting and ending points of the muscles is very helpful for the sticking and rehabilitation.
What is the lips?
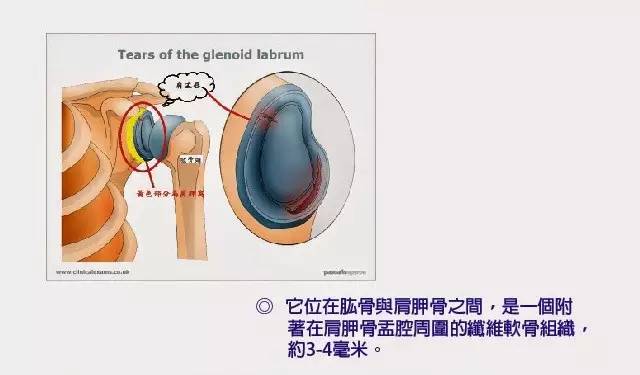
Q: Why do you know that lip is important?
A: Because the shoulder joint is classified as a ball and socket joint, in fact, the shoulder armpit is very shallow and can only cover one third of the humeral head. The other parts can only be wrapped by the lips, which can stabilize the shoulder. .
What are the injuries of the biceps tendon?
2. Early shoulder movements are not significantly restricted, but pain during abduction, extension, and rotation. Gradually increased, shoulder movements are limited, and the affected hand cannot touch the contralateral scapula.
3. The tenderness of the intercondylar sulcus is obvious.
4. The biceps resistance test (Yergason sign) is positive: in the case of resistance, when the elbow and forearm are supinated, severe pain occurs around the biceps tendon.
5. Patients with frozen shoulder or other diseases have a wide range of pain, showing shoulder stiffness and muscle atrophy.
The way you can work hard
Non-surgical treatment of biceps tendon tenosynovitis can be effective, such as reducing hand activity, applying traditional Chinese medicine safflower oil and other blood-activating and swelling drugs, applying plaster, oral non-steroidal anti-inflammatory drugs. If necessary, local closure treatment can be used to inject 0.5 to 1 ml of lidocaine and triamcinolone acetonide into the tendon sheath. The early one can be effective, and the stubborn one can be once a week, no more than 4 Times.
(1) Those with severe local brake pain can use the triangle towel to suspend the forearm; avoid excessive use of the shoulder joint.
(2) Partially closed in the most obvious position of the biceps muscle groove tenderness, first inject 1% procaine 5ml, then intraperitoneal injection of hydrocortisone acetate or prednisolone 1ml (25mg), weekly Once, it can be used 1 to 3 times. Strict aseptic operation is required. Most of the effects are significant. Some patients may have a slight increase in symptoms due to drug reaction within 3 days of injection.
(3) After the exercise is relieved of pain, exercise is performed to prevent the frozen shoulder from occurring. 1 Shoulder active activity: bending over to make the affected limb relax and sag, doing shoulder swinging exercise, many times a day. 2 climbing wall movement: the hand moves up the wall, gradually recovering the shoulder abduction and lifting. 3 pulley with arm lifting method: both hands pull the two ends of the pulley rope mounted on the wall, sliding up and down to restore shoulder outreach activities.
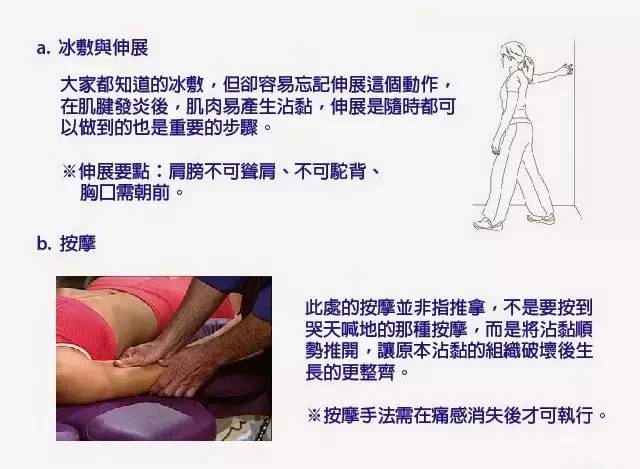
(4) Massage massage uses squatting, holding, pinching, rolling, trembling and other techniques to passively move the shoulder joint to improve local blood supply and promote functional recovery.
(5) Local physiotherapy or hot compress local physiotherapy or hot compress helps the inflammation to subside.
(6) Taking anti-inflammatory and analgesic drugs can reduce pain by taking anti-inflammatory and analgesic drugs. A new class of anti-inflammatory analgesics has better effects and fewer side effects.
2. Surgical therapy
Surgical therapy is indicated for individual cases of refractory biceps tendonitis. Severe pain, joint activity is significantly limited, after more than half a year of non-surgical treatment, surgery can be considered. The method is to cut the biceps tendon of the biceps muscle under the nodular groove, and the distal end is sutured with the biceps brachial brevis or fixed on the humerus to eliminate the friction of the tendon and relieve the symptoms. After the operation, the upper limbs were bandaged for 2 weeks, and then physical exercise began. A small number of patients who need surgery, antibiotics should be used after surgery. Choose different antibiotics depending on the situation.
Overbed/laptop table is the most versatile, feature-packed table available today. Hollin earned its name due to its extreme versatility and high level of functionality. The rugged, institutional quality design and construction combined with the most-desired user features makes the Hollin is perfect fit for home and institutional healthcare use as well as an ideal Laptop Cart for home or office. Hollin can integrate with more bed/chair shapes and sizes than any other overbed table on the market. The split top design allows the user to tilt the main table surface in either direction for easier book/tablet reading while a smaller fixed surface remains horizontal to accommodate. pen/paper/drinks/food/mousepad and mouse etc. An integrated lip prevents items placed on the tilted surface from sliding off. Hollin table can be easily and conveniently stored in a very small area. The storage mode also makes the easy to transport if required.
Overbed Table,Laptop Lap Desk,Bed Laptop Desk,Ikea Laptop Desk,Over Bed Table
Foshan Hollin Furniture Co.,Ltd , https://www.foshanhollin.com